Table-Mounted Retractor Options for Long Thoracoabdominal Aortic Procedures
Thoracoabdominal aortic aneurysm (TAAA) procedures place sustained demands on surgical exposure. These cases extend across thoracic and abdominal regions, often over multiple hours, with access requirements that change as the procedure progresses. Maintaining consistent exposure depends on how well the retractor set performs under load, at depth, and throughout the entire procedure.
Selecting the right type of retraction in these procedures focuses on the overall approach rather than on an individual retractor. Table-mounted retractor sets provide a stable, hands-free foundation that supports multi-plane exposure, controlled adjustments, and workflow continuity throughout long-duration vascular cases.
Why TAAA Procedures Require Specialized Retraction
TAAA repair combines depth, duration, and anatomical complexity. Exposure often begins in one region and extends into another, requiring access across both thoracic and abdominal phases without interrupting the operative field.
These procedures introduce several consistent challenges:
● Deep operative fields requiring extended reach into retroperitoneal and thoracic spaces
● Multi-quadrant access where exposure must be maintained across a broad surgical area
● Shifting anatomy as dissection progresses and access vectors change
● Extended operative time where retraction must hold position for hours without drift
In hybrid or staged procedures, exposure demands become even more dynamic. Surgeons may transition between open and endovascular components, requiring stable access during imaging, device placement, and potential conversion.
In this environment, retraction is not static. It must maintain consistent geometry under sustained load while allowing controlled refinement as the case evolves. This is why table-mounted retractor sets are commonly used in TAAA procedures; they provide a stable base that supports both long-duration exposure and incremental adjustment without repeated repositioning.
Core Categories of Retractor Options for TAAA
Retractor options for long thoracoabdominal procedures are best understood as combinations of structural components rather than as standalone tools. Performance depends on how the frame, arms, and blades work together to create and maintain exposure.
Table-Mounted Frame-Based Retractor Sets
Table-mounted retractor sets form the foundation of retraction in TAAA procedures. By anchoring directly to the operating room bedrail, these sets create a stable base that resists flex, drift, and gradual loss of tension in deep operative fields.
Frame rigidity is a primary consideration. In long cases, even small geometric shifts can compromise visualization and require mid-case correction. A rigid, table-mounted frame distributes retraction forces across the construct rather than concentrating tension at a single point, allowing exposure to remain stable over extended durations.
Because the frame remains fixed to the table, surgical teams can maintain consistent access without relying on continuous manual retraction. This supports hands-free operation and reduces variability during multi-hour procedures.
Modular Frame Configurations (OneFrame, Quick Frame, RingTrack)
Within table-mounted retraction, different frame configurations are used to support specific exposure strategies.
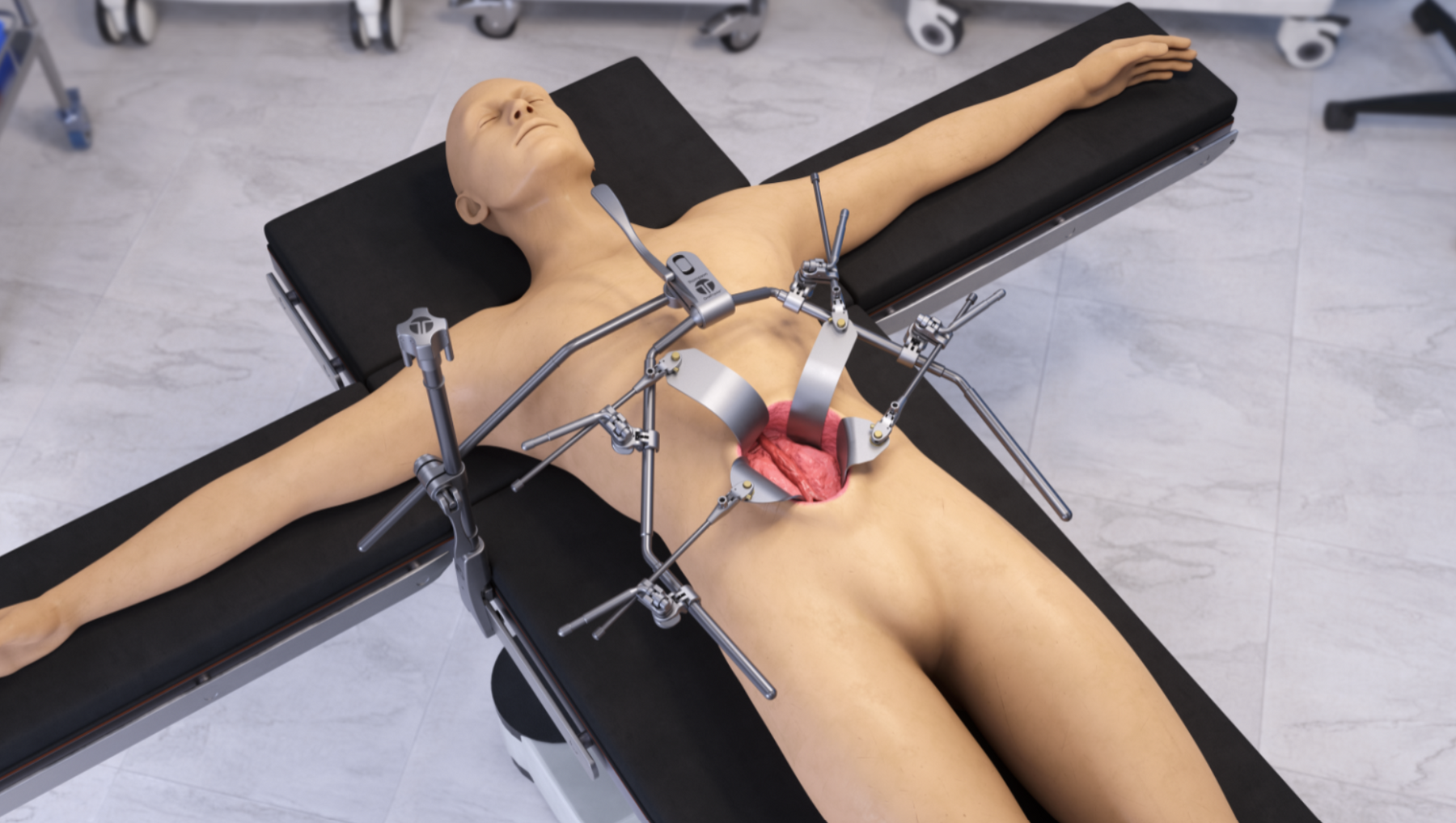
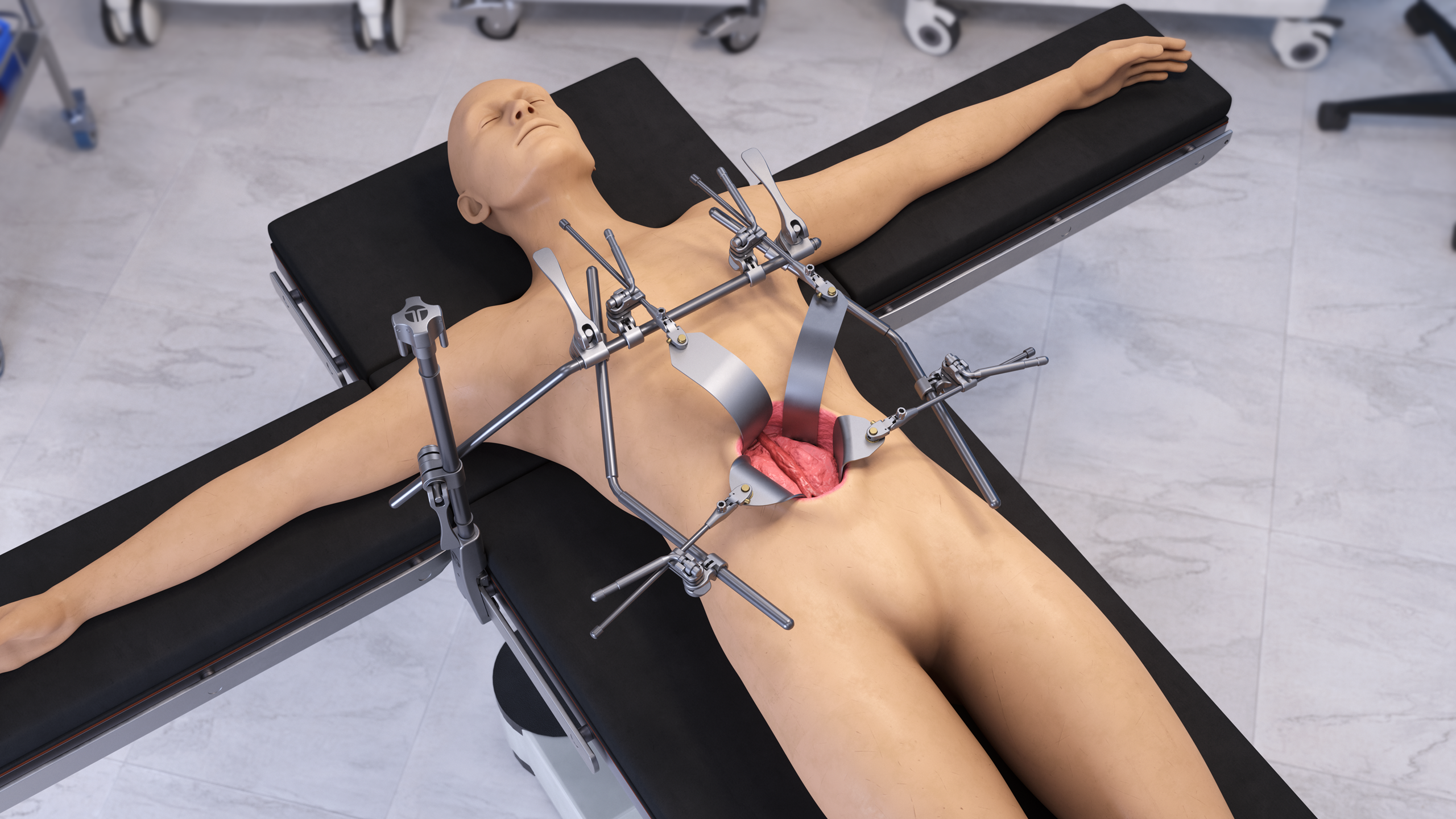
● OneFrame configurations are designed for rigid, multiplanar access in deep abdominal and retroperitoneal exposure. The structure supports stable positioning while allowing adjustable arm placement across the frame.
● Quick Frame configurations provide a simplified, efficient structure that supports rapid setup and adjustment, often used in procedures where flexibility and speed are important without sacrificing stability.
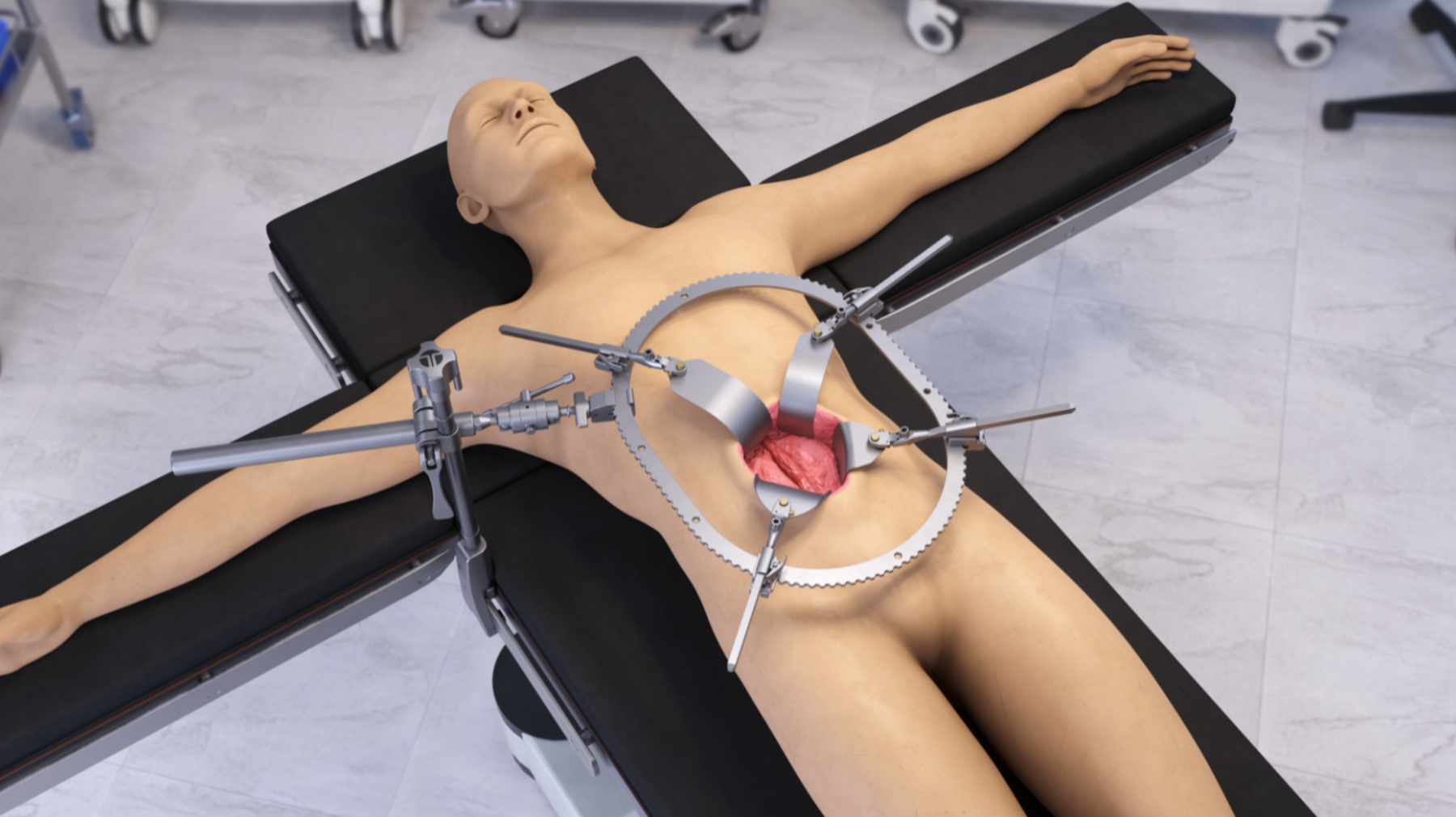
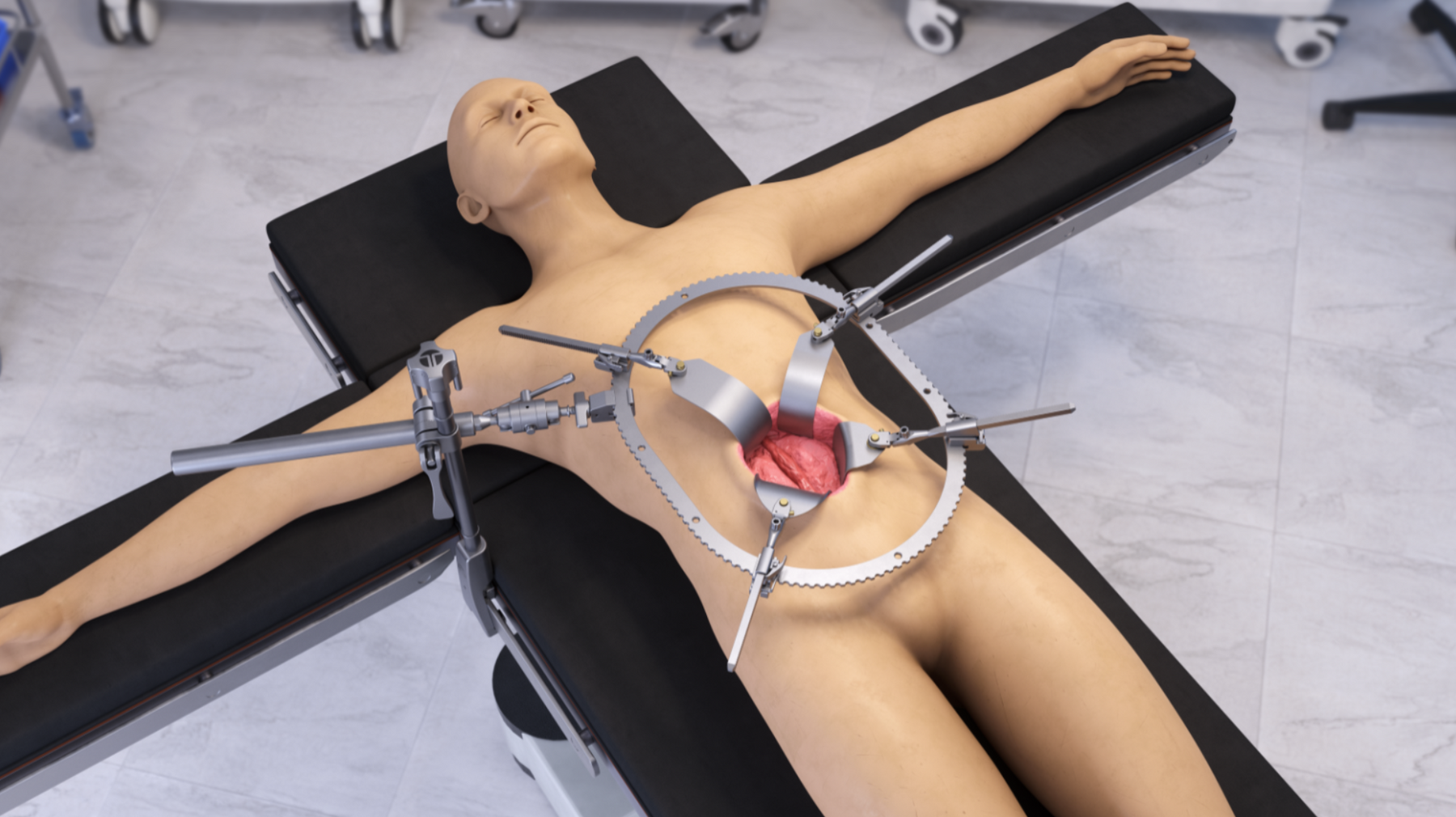
● RingTrack configurations use a ratcheted ring-style frame that allows retraction points to be positioned around the operative field. This supports circumferential access and allows blades to be repositioned along the frame without rebuilding the setup.
Each configuration serves a different purpose, but all operate within the same table-mounted approach. The primary advantage is the ability to adapt the retractor set to the procedural requirements while maintaining a stable foundation.
Arm Positioning and Multi-Planar Control
Combined thoracoabdominal procedures rarely require retraction in a single direction. Access may shift as the procedure progresses, requiring adjustments in depth, angle, and direction of pull.
Retractor sets for TAAA exposure support independent arm positioning, allowing surgical teams to control each retraction point separately. This enables:
● Directional control across multiple planes
● Localized adjustments without disrupting the overall construct
● Incremental refinement as access deepens or shifts
Rather than dismantling and rebuilding the retraction setup, teams can adjust individual components while maintaining the overall geometry of the operative field. This supports workflow continuity and reduces interruptions during long-duration procedures.
Blade Ecosystem: What Determines Performance in TAAA Exposure
In long thoracoabdominal procedures, blade selection directly determines how effectively exposure is created and maintained at depth. As access extends into retroperitoneal and upper abdominal regions, blade length, contour, and engagement behavior all influence visibility and control.
A well-developed blade ecosystem allows surgical teams to match retraction to anatomy and procedural phase, rather than forcing a single configuration to work across all conditions.
Key blade characteristics to evaluate include:
● Extended reach to support deep retroperitoneal and subdiaphragmatic access
● Width and contour options to distribute force and match the incision strategy
● Malleability, allowing blades to be shaped when needed to accommodate anatomy
● Angle of engagement, supporting a clear operative corridor without obstructing the field
● Locking behavior, determining whether retraction holds a fixed plane or adapts under tension
In long-duration vascular procedures, these factors affect not only initial exposure, but how consistently that exposure is maintained as tissue shifts and access deepens.
Within table-mounted retractor sets, blade interface design plays a key role in how retraction behaves over time. Two commonly used configurations include:
● S-Lock® (SL) blades, which allow positioning and then lock into a fixed plane when consistent directional retraction is required
● Swivel-Only (SO) blades, which align naturally with patient anatomy under sustained tension, supporting adaptive engagement
This combination allows surgical teams to choose between controlled, fixed retraction and more flexible, anatomy-following behavior depending on the demands of each phase of the procedure.
In TAAA cases, where exposure evolves over time, the ability to select and adjust blade configurations allows teams to refine access without rebuilding the retraction construct.
Building Retraction for Multi-Phase TAAA Procedures
Thoracoabdominal aortic procedures rarely rely on a single, static retraction setup. Instead, surgical teams often approach retraction as a structured configuration that can support different phases of the case while maintaining a stable foundation.
This approach is commonly built around defined exposure “modules,” which allow teams to standardize key elements of retraction while preserving flexibility for patient-specific anatomy.
Typical configurations may include:
● A thoracic component, coordinated with rib spreading to establish initial access
● A table-mounted abdominal component, supporting deep retroperitoneal and multi-quadrant exposure
● Blade selections matched to the depth and direction of pull for each phase
● Arm positioning patterns that define consistent retraction vectors
By defining these elements in advance, teams avoid having to rebuild the retractor set from scratch during the procedure. Instead, they establish a stable construct and make targeted adjustments as access requirements change.
Preference cards play a central role in this process. In long aortic cases, they define not only which components are used, but also how the retraction set is assembled and positioned. When consistently applied, this creates a repeatable setup that reduces variability between cases and across teams.
As the procedure progresses, exposure demands inevitably shift. Depth increases, anatomical focus changes, and access vectors adjust. Retraction sets designed for TAAA procedures support:
● Localized arm repositioning without full disassembly
● Blade exchanges without disturbing the base construct
● Incremental adjustments rather than full resets
This allows surgical teams to refine exposure while maintaining the overall geometry of the operative field.
In multi-hour vascular procedures, this distinction is critical. When the foundational retractor construct remains stable and predictable, adjustments become controlled and efficient rather than disruptive. The result is fewer workflow interruptions and more consistent surgical access across both thoracic and abdominal phases.
Retraction in Hybrid and Endovascular TAAA Procedures
Thoracoabdominal aortic repair has evolved to include hybrid and endovascular techniques, but these approaches have not eliminated the need for controlled open exposure. In many cases, surgeons move between catheter-based steps and open surgical components within the same procedure or across staged interventions.
This shift has changed how retraction is used. Exposure is no longer linear. Instead, it must support transitions between:
● Open dissection and vessel control
● Imaging and device positioning
● Additional access for debranching or graft work
● Potential conversion from endovascular to open techniques
These transitions require a retraction approach that remains stable while the procedure evolves. The operative field must accommodate imaging equipment, device manipulation, and surgical access without losing exposure or obstructing the working corridor.
Table-mounted retractor sets are commonly used in this setting because they provide a fixed foundation that supports controlled modification. Instead of resetting handheld retractors during each phase, teams can refine access incrementally while maintaining overall stability.
In hybrid procedures, dependable retraction does not compete with endovascular technology; it supports it. Stable exposure allows surgeons to maintain access for vascular control, device placement, and contingency planning without interrupting workflow.
Evaluating Retractor Options for Long TAAA Procedures
Selecting retractor options for thoracoabdominal procedures requires a structured evaluation approach. Performance in these cases is determined by how well the retractor set maintains stability, supports adjustment, and integrates into the surgical workflow over time.
A practical evaluation framework includes five core categories:
Frame Rigidity
The frame must resist flex, drift, and loss of tension under sustained retraction. In deep operative fields, even small shifts can compromise visualization and require correction.
Arm Adjustability
Arms should support independent positioning, allowing directional control and localized adjustments without disrupting the overall construct.
Blade Ecosystem
Blade length, contour, and interface determine how effectively deep access is maintained. A range of options is required to match the anatomy and the procedural phase.
OR Footprint and Workflow Impact
Retractor sets should preserve working space and avoid obstructing instruments, assistants, or imaging equipment within the operative field.
Turnover and Sterile Processing Considerations
Modular components must support efficient disassembly, inspection, and reprocessing to maintain consistency between cases.
When these elements are evaluated together, surgical teams can identify retractor sets designed for long-duration vascular procedures rather than short, isolated exposures.
OR Footprint and Workflow Considerations
Thoracoabdominal procedures require space for multiple instruments, assistants, suction devices, and monitoring equipment. Retraction affects not only exposure, but also how that space is used.
Frame design and placement determine whether the operative field remains accessible or becomes crowded. In deep abdominal and retroperitoneal access, maintaining a clear working corridor is essential for both visualization and instrument handling.
Key considerations include:
● Frame size relative to the incision and operative field
● Placement of structural components outside the central working area
● Accessibility of adjustment points without entering the incision field
● Compatibility with thoracic access tools, such as rib spreaders
Table-mounted retractor sets support this by anchoring to the OR bedrail, positioning structural support outside the primary surgical corridor. This allows teams to maintain stable exposure while preserving usable space for instruments and procedural steps.
In long vascular cases, preserving the working environment is as important as maintaining exposure itself.
Sterile Processing and Turnover Considerations
In long thoracoabdominal procedures, retractor sets are exposed to extended operative time, heavy tissue load, and complex configurations. Performance in the next case depends on how consistently those components are cleaned, inspected, and reassembled.
Large table-mounted retractor sets typically include:
● Frame components and crossbars
● Multiple articulated arms
● Blade handles and locking interfaces
● A range of blade lengths and profiles
After extended procedures, these components often require detailed cleaning, particularly at joints, locking mechanisms, and blade interfaces. Without a standardized approach, variability in processing can affect both turnaround time and performance consistency.
Effective turnover depends on:
● Defined disassembly sequences
● Consistent inspection of joints and locking interfaces
● Proper lubrication where required
● Standardized tray configurations aligned with preference cards
When retractor sets are processed and rebuilt consistently, they return to the operating room in a predictable configuration. This supports reliable setup and reduces delays in high-acuity surgical schedules.
In long aortic cases, consistency in sterile processing is not separate from surgical performance; it directly supports it.
Why Table-Mounted Retraction Remains the Standard for TAAA
Across all variations in thoracoabdominal aortic repair—open, hybrid, or staged—one requirement remains consistent: exposure must be stable, controlled, and adaptable over time.
Table-mounted retractor sets meet this requirement by providing:
● A stable base anchored to the operating table
● Hands-free retraction maintained over extended durations
● Multi-planed control for evolving access needs
● Modular configurations that adapt without disrupting the operative field
In long TAAA procedures, these characteristics allow retraction to serve as a dependable foundation rather than a variable requiring constant correction.
Choosing the Right Retractor Set for TAAA Procedures
Selecting the right retractor set depends on the specific demands of the procedure, including anatomical complexity, depth of access, and workflow requirements.
Rather than focusing on a single configuration, surgical teams evaluate how a table-mounted platform can be adapted through:
● Frame selection
● Arm positioning
● Blade configuration
This approach allows teams to standardize around a stable foundation while maintaining flexibility for procedural variation.
When these elements are aligned, retraction supports consistent exposure across thoracic and abdominal phases, reduces variability between cases, and improves workflow continuity during extended vascular procedures.
Evaluate Table-Mounted Retraction in Your OR
Thompson Surgical Instruments designs table-mounted retractor sets built for long, complex procedures, including thoracoabdominal aortic repair. These sets are engineered to provide stable, hands-free retraction, modular configurability, and consistent performance across extended operative durations.
Surgical teams can evaluate configurations through a 30-day clinical trial that includes training and case support. This allows teams to assess how retraction performs within their own workflow and procedural environment.
Thompson Surgical Instruments engineers table-mounted retractor sets designed to support stable, hands-free exposure in long thoracoabdominal aortic procedures. We provide modular configurations, blade options, and clinical support to help surgical teams maintain consistent access across complex, multi-phase cases. Contact us today to learn more about retractors for long TAAA surgeries.

Share:
Pelvic & GYN Oncology Exposure: Optimizing Deep, Stable Retraction for Complex Resections