
Thoracoabdominal aortic repair increasingly incorporates hybrid and endovascular techniques, including fenestrated and branched devices. Even when minimally invasive strategies are used, surgeons often require dependable open surgical access for debranching, vascular control, or unexpected conversion. Stable, table-mounted retraction remains critical when sustained exposure is required during these complex procedures.
The Evolution of Thoracoabdominal Aortic Repair
Thoracoabdominal aortic aneurysm (TAAA) repair has evolved significantly over the past two decades. Advances in imaging, engineering, endovascular devices, and catheter-based therapies have expanded the range of treatment options beyond traditional open repair. Surgeons now routinely evaluate patients for fenestrated and branched endografts, staged repairs, and hybrid approaches that combine open and endovascular techniques.
These innovations have reduced the invasiveness of certain procedural components. However, they have also increased procedural complexity. Many thoracoabdominal repairs now require coordination between imaging guidance, catheter-based device deployment, and precise surgical exposure. Rather than replacing open techniques entirely, modern strategies often integrate open and endovascular elements within the same case or across staged interventions.
As a result, exposure planning has become more nuanced. Surgical teams must anticipate when minimally invasive steps may transition to open components, particularly in long or anatomically complex procedures.
The Rise of Hybrid and Innovative Endovascular Devices in TAAA Repair
Endovascular devices are minimally invasive, catheter-delivered tools, including stents, balloons, grafts, and guidewires, designed to treat vascular disease from inside the blood vessel. In thoracoabdominal repair, fenestrated and branched stent grafts allow surgeons to maintain perfusion to vital branch vessels while excluding aneurysmal segments of the aorta.
Hybrid repair strategies often combine open surgical debranching with endovascular graft placement. For example, visceral or renal vessels may be surgically reimplanted or bypassed before placement of an endograft. This blended approach can reduce certain physiologic stresses compared to fully open repair while still requiring direct surgical access during critical phases.
These approaches demand precision and coordination. Imaging, device positioning, and vascular control must align. While some portions of the procedure may be catheter-based, others still require controlled, stable open surgical access to deep retroperitoneal or thoracoabdominal fields. For this reason, exposure strategy remains central, even in the era of advanced endovascular technology.
Why Open Surgical Access Still Matters in Hybrid Aortic Repair
Hybrid and endovascular techniques do not eliminate the need for open surgical access. In many thoracoabdominal cases, surgeons must still perform open exposure for debranching, vessel control, graft sewing, or direct visualization. Even procedures initially planned as endovascular may require open conversion if device deployment challenges arise.
In long thoracoabdominal repairs, depth and anatomical complexity remain constant regardless of delivery method. Large vessels, branch arteries, and adjacent structures must be precisely identified and controlled. When portions of the case transition from catheter-based steps to direct surgical manipulation, exposure must already be secure and dependable.
This is where the exposure strategy becomes strategic rather than incidental. Surgical teams develop retraction plans that support both open components and potential intraoperative adjustments without destabilizing the operative field.
How Hybrid Approaches Change Exposure Demands
As hybrid procedures become more common, exposure demands become less linear and more dynamic. Traditional open thoracoabdominal cases typically progressed in a defined exposure sequence. Hybrid procedures, by contrast, may alternate between open dissection, device positioning, imaging verification, and additional vessel work.
Retraction sets must support:
● Variable depth across thoracic and abdominal zones
● Shifting vectors of pull as anatomical focus changes
● Unobstructed workspace during device manipulation
● Stable access during imaging-dependent steps
● Rapid re-adjustment without full reconfiguration
In multi-hour vascular procedures, the ability to make localized retraction adjustments without disrupting the broader construct becomes critical. Exposure must remain controlled while workflow evolves.
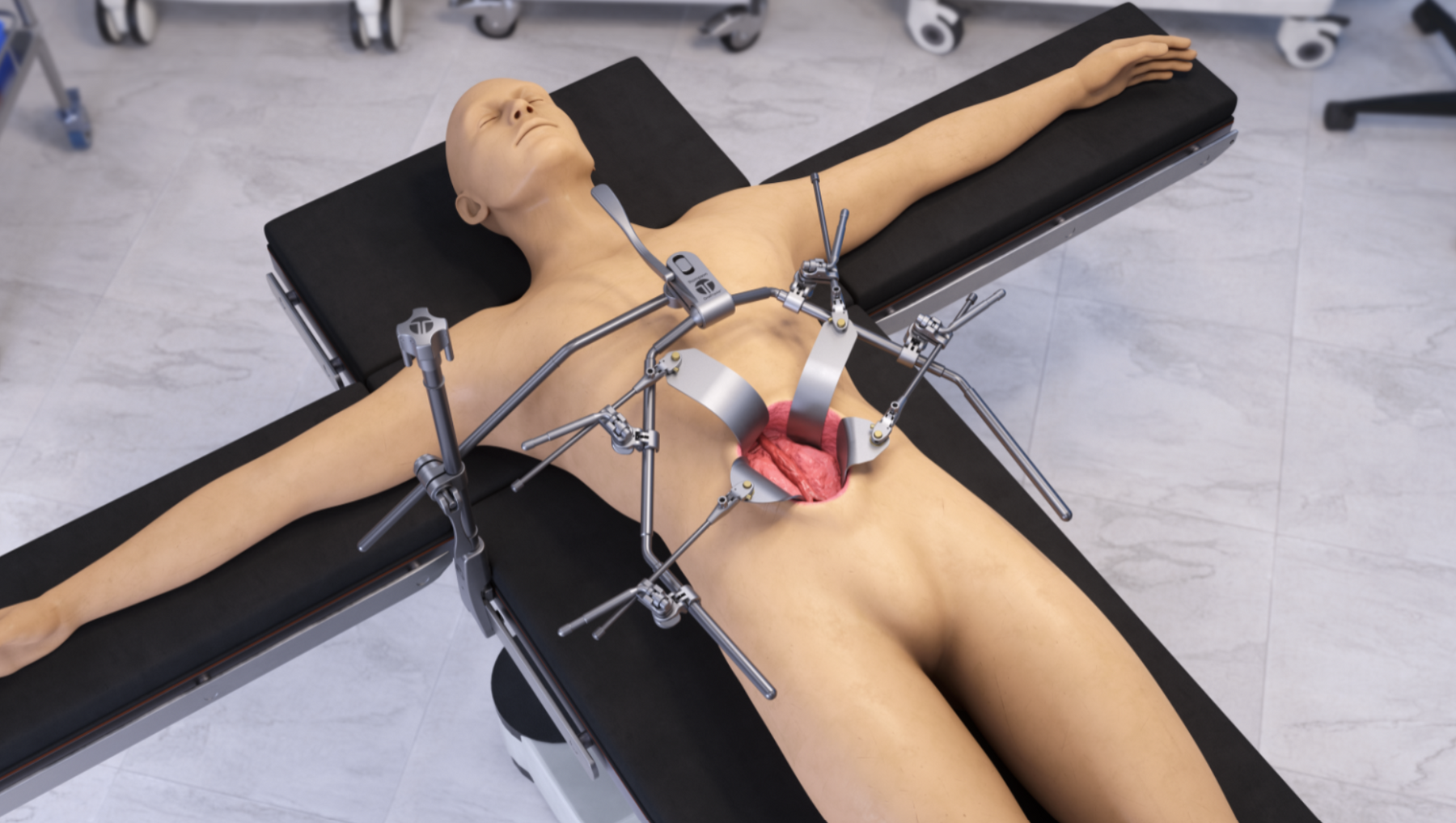
Table-mounted retraction sets are often selected in this setting because they anchor directly to the operating table, providing a stable base for controlled modification. Instead of repeatedly resetting handheld retractors, teams can fine-tune surgical access while maintaining core stability.
The Role of Table-Mounted Retraction in Modern Thoracoabdominal Repair
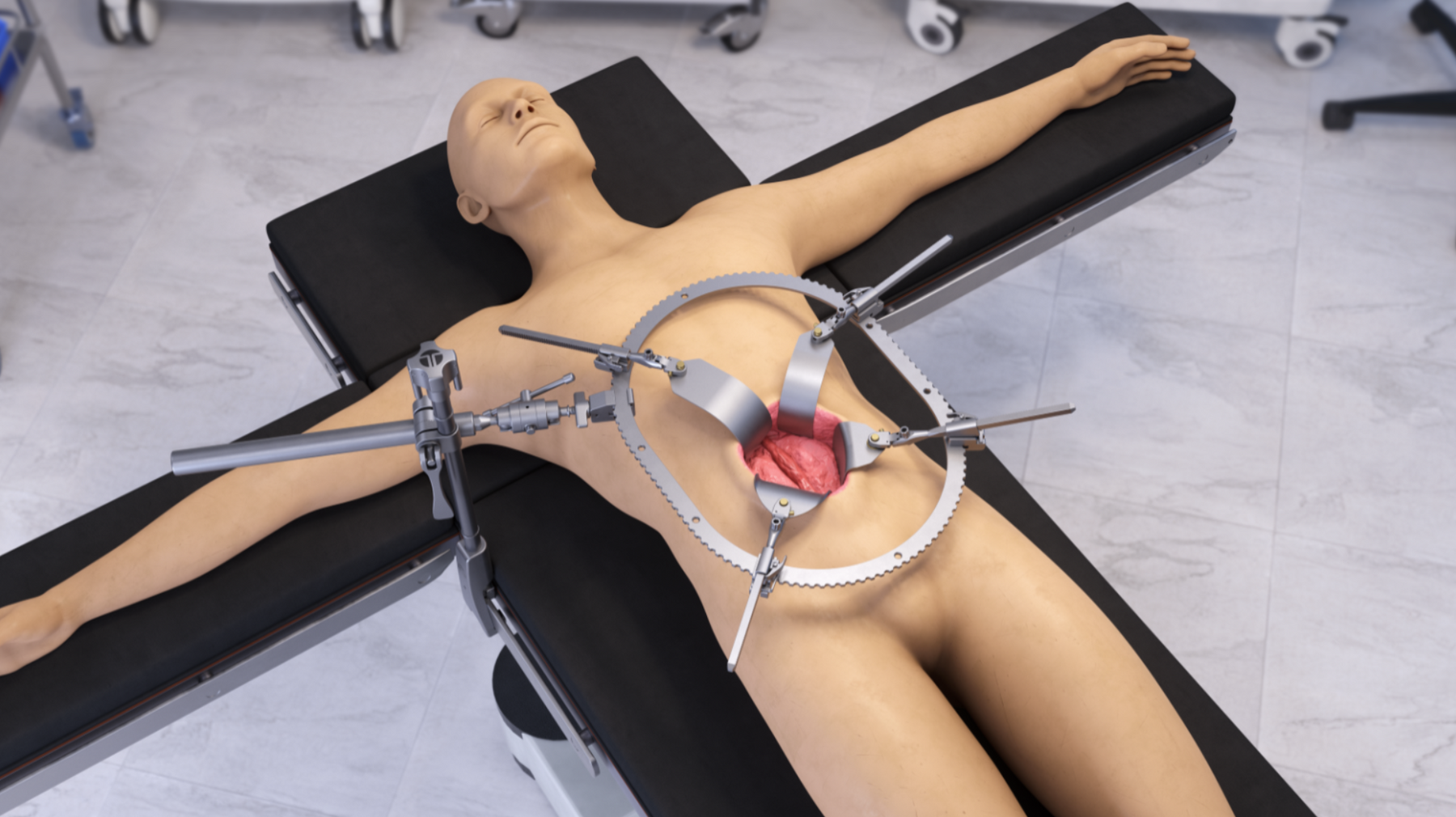
Table-mounted retraction provides hands-free support anchored to the OR bedrail, creating a mechanical foundation designed to resist drift under sustained tension. In hybrid thoracoabdominal repair, this stability supports deep operative access during prolonged open components and potential conversion scenarios.
Key advantages of table-mounted retraction in hybrid cases include:
● Sustained stability during long-duration exposure
● Multi-planed control to accommodate changing anatomical focus
● Reduced reliance on continuous manual holding
● Improved workspace management during device deployment
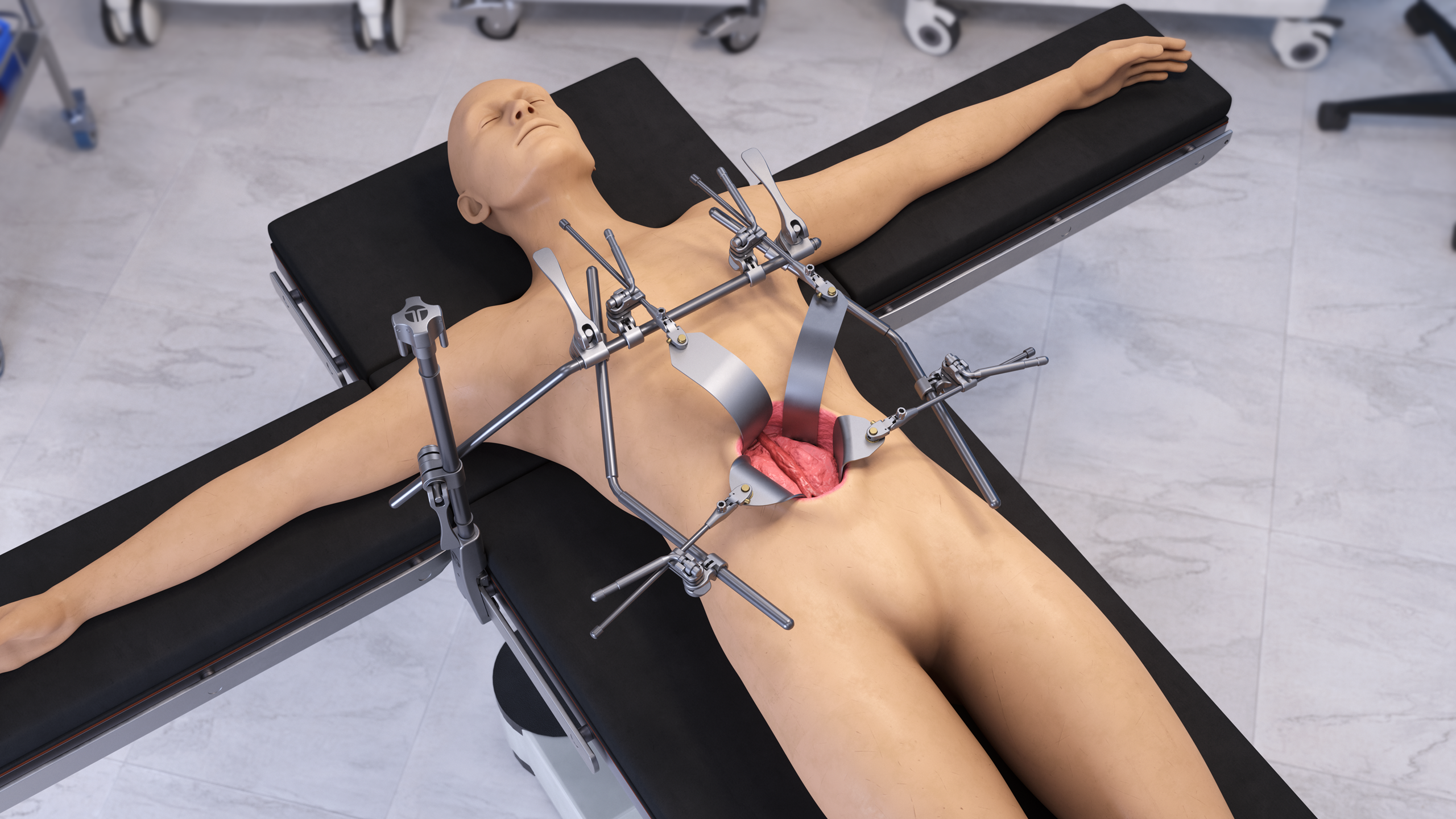
As imaging tools and catheter-based devices are positioned, the surgical field must remain accessible without crowding the operative corridor. A stable, anchored retraction set allows surgeons to maintain surgical access while other technologies are introduced into the field.
Rather than competing with endovascular innovation, dependable retraction supports it. Controlled access enables vascular control, precise vessel handling, and orderly workflow during combined techniques.
Planning for Conversion: Building Exposure into Contingency Strategy
Even with advanced endovascular devices, thoracoabdominal procedures carry inherent variability. Anatomical challenges, calcification, device positioning difficulties, or unforeseen bleeding may require escalation to open techniques.
Experienced vascular teams plan for this possibility in advance. Exposure is not treated as a backup; it is integrated into the operative strategy from the outset. Stable table-mounted retraction sets allow teams to maintain readiness without disrupting the flow of the minimally invasive component.
By standardizing retraction setups that can accommodate both open and hybrid phases, surgical teams reduce intra-case delays and improve procedural confidence. Access planning becomes part of risk management rather than a reactive measure.
How Thompson Surgical Instruments Supports Modern Aortic Access
For more than 60 years, Thompson Surgical Instruments has focused exclusively on table-mounted retraction sets designed to support stable, hands-free surgical access across specialties. In complex thoracoabdominal cases, stability, configurability, and repeatability remain central to exposure success.
Thompson retractor sets provide:
● Anchored, table-mounted stability designed for prolonged procedures
● Modular frame configurations are adaptable to thoracic and abdominal access
● Multi-planed control through articulating arms
● A blade ecosystem featuring S-Lock® (SL) and Swivel-Only (SO) options to support either fixed-plane retraction or anatomy-following alignment
By combining structural stability with configurable blade options, Thompson retractor sets allow teams to refine surgical exposure based on anatomy, depth, and procedural phase. In the evolving landscape of hybrid and open aortic repair, dependable surgical access remains a constant requirement.
Innovation Alters Methods, Yet Reliable Surgical Access Remains Essential
Thoracoabdominal aortic repair continues to evolve as hybrid and endovascular device technologies expand treatment possibilities. Fenestrated and branched devices offer new solutions, but they do not eliminate the need for controlled open exposure during critical phases of complex procedures. In many cases, minimally invasive techniques increase procedural coordination demands rather than simplify them.
As hybrid strategies grow, exposure planning becomes even more deliberate. Surgical teams must anticipate transitions between open and endovascular components, maintain stability during device deployment, and prepare for contingency scenarios without interrupting workflow. Dependable table-mounted retraction remains foundational in this environment, supporting sustained surgical access while other technologies evolve around it.
Innovation may change how vascular repair is performed, but consistent, stable access to the operative field remains a constant requirement in long thoracoabdominal procedures.
For over 60 years, Thompson Surgical Instruments has advanced table-mounted retraction sets guided by our mission of the Relentless Pursuit of Perfection, delivering stable, configurable solutions surgeons rely on in complex procedures worldwide. As the inventor of the first patented table-mounted retractor in 1965 and the sole manufacturer of the Thompson Retractor, our employee-owned team continues to refine retractors engineered for durability, precision, and dependable performance. Contact us to learn how Thompson Surgical Instruments supports modern innovation of endovascular devices with consistent surgical access.

Share:
Standardizing Retraction for Multi-Hour Aortic Surgeries: How Teams Build Repeatable Setups (Without Reinventing the Wheel)
Liver, Transplant, and Complex Upper-Abdominal Oncology: Why Bilateral Retraction is Popular